Sleep and Treatments in Insomnia - Pharmacy Times
Introduction
Sleep is a vital component for the human body. If left untreated, sleep disorders such as insomnia can lead to other health problems.
Pharmacists play a role in providing consumers with recommendations on OTC and herbal remedies to manage insomnia. Pharmacists also provide drug information to prescribers and guide appropriate prescription drug use.
Presently there are several prescription drug classes that can be used to increase sleep latency and/or sleep duration. Benzodiazepines, Z drugs, melatonin receptor agonists, and orexin receptor antagonists are used in treating insomnia.
Specific antidepressants, anticonvulsants, and atypical antipsychotics are used off label to manage insomnia. Research on chemicals and receptors in the brain and their effects on sleep continue to be an area of growth in the development of new drugs for sleep disorders.
Epidemiology and Statistics
The National Sleep Foundation Survey in the United States found that 75% of US adults have at least 1 symptom of a sleep disorder and 54% have 1 symptom of insomnia. Americans spend an estimated $2 billion every year on sleep medications.1
One of the goals of Healthy People 2030 includes increasing the number of adults and young adults who get enough sleep.2 Globally, samples from different countries indicate a prevalence rate of insomnia of about 30% to 40% in the general population.3 These cases report difficulty initiating sleep, difficulty maintaining sleep, waking up too early, and, in some cases, non-restorative or poor quality sleep.3
The Brain and Sleep
What happens in the brain when we sleep? Melatonin, a hormone secreted by the pineal gland in the brain, peaks in the late evening in response to changes in light and darkness. This hormone regulates circadian rhythms, which are the 24-hour physiologic patterns of sleep and wakefulness.1
Researchers have studied the brain and have classified sleep into 2 types: non-rapid eye movement (N) sleep and rapid eye movement (REM) sleep. N sleep is also known as quiet sleep and can be further classified as stages N1, N2, and N3.
During N sleep, thinking and physiological activities slow down. Approximately 5 minutes is spent on making the transition from wakefulness to light sleep, which is called N1 sleep. The reading on an electroencephalogram (EEG) depicts theta waves that are spread apart (Figure 1).
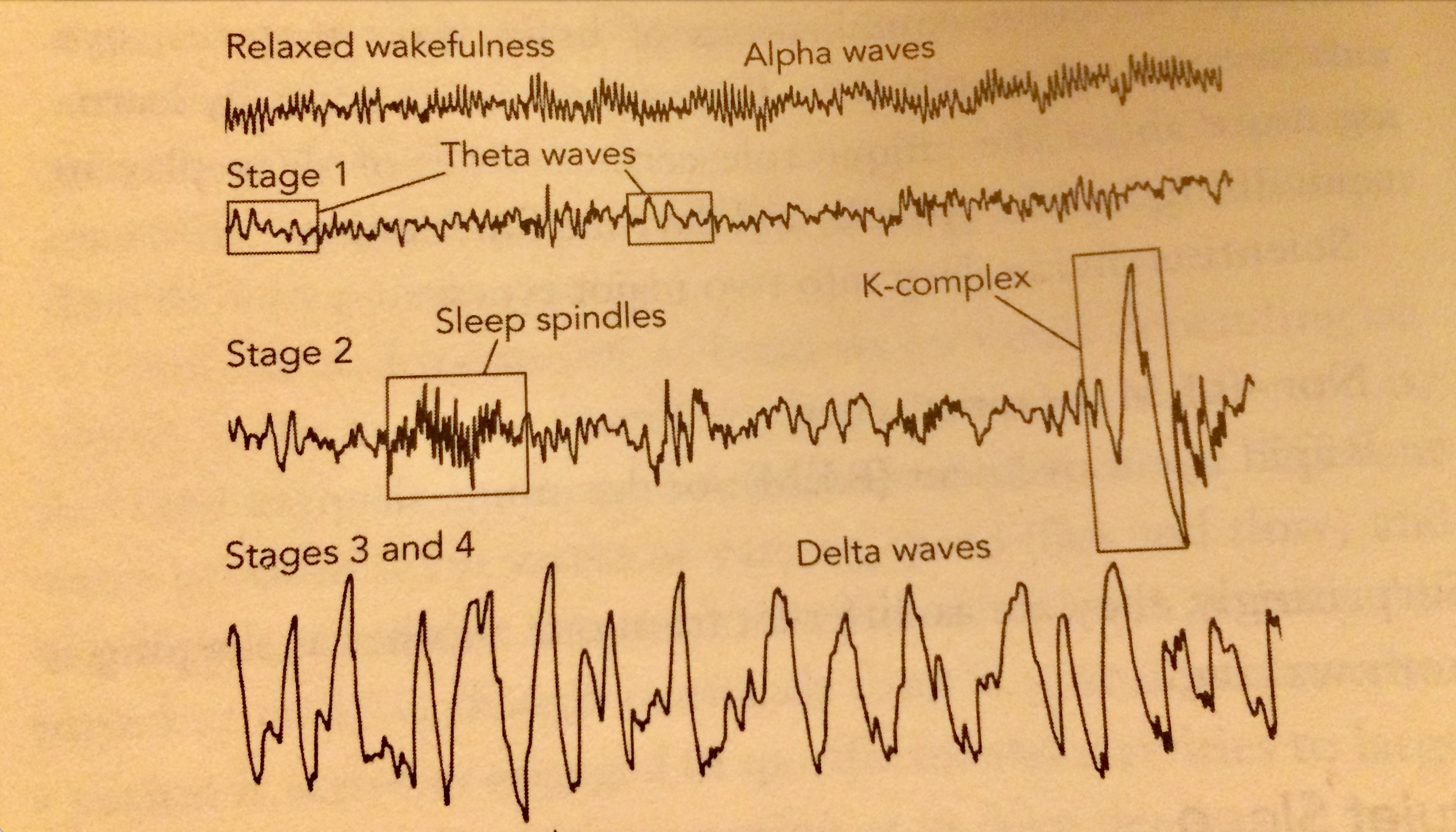
Credit: Epstein, L., & Mardon S., The Harvard Medical School Guide to a good night's sleep, New York: McGraw Hill, 2007.
Body temperature decreases and muscles become relaxed. The eyes move slowly from side to side and one can easily awaken. In N2 sleep, which lasts 10 to 25 minutes, heart rate and breathing slow down. Fifty percent of your sleep at night is spent in N2. EEG depicts sleep spindles and K complexes (Figure 1).
N3 sleep is known as deep sleep. EEG depicts deep delta waves sometimes referred to as slow wave sleep (SWS). During deep sleep, your breathing slows down and becomes more regular.
Blood pressure and pulse decrease to about 20% to 30% below waking rates. Deep sleep is when your body renews and repairs itself. Less blood flow occurs to the brain.
The pituitary gland releases growth hormone that stimulates tissue and muscle repair. Researchers have discovered that interleukin—a chemical that activates the immune system—increases during deep sleep, which suggests that deep sleep may defend against infection.4
REM sleep depicts brain activity including theta waves on an EEG. During REM sleep, blood pressure, heart, and respiratory rate increase and dreaming occurs. REM sleep, which facilitates learning and memory, comprises approximately 25% of total sleep time. Every 90 minutes a sleeper will enter REM sleep.
Finally, sleep is an important function for the human body. During REM and N sleep, body temperature, blood pressure, digestive enzymes, urine production, and sleep and wakefulness are being regulated.4
Aging and Sleep
As we age, sleep patterns tend to change. Newborns sleep 12 to 19 hours a day, which includes a few minutes of sleep to several hours of sleep. Half of the time is spent in quiet sleep and the rest in REM sleep.
During infancy sleeping patterns become more regular. At 6 months of age, most infants sleep throughout the night and nap during the day. From age 1 to 3, sleep ranges from 12 to 14 hours a day.
Toddlers can experience sleep disturbances such as nighttime awakenings and nightmares. At 3 to 5 years of age, sleep length decreases to 11 to 13 hours a day. Preschoolers can have nighttime awakenings, sleepwalking, sleep terrors, and bedwetting.
From 6 years to puberty, adult sleep patterns begin to develop. Melatonin production is at its highest level in this age group and children fall asleep easily. Eleven hours of sleep is usually required; however, most in this age group sleep approximately 8 hours.
Bedwetting, nightmares, and sleepwalking decrease during adolescence, and there is rapid body growth and development. Adolescent sleep patterns include going to bed late and sleeping late. This age group typically requires 10 hours of sleep.1
Most adults need 7.5 to 8 hours of sleep per night to function well; however, as we age, sleep latency, the time it takes to fall asleep, increases. Total nighttime sleep or sleep duration decreases each decade as we age.
From 20 to 40 years of age, sleep latency is approximately 16 minutes and sleep duration 7.5 hours. From 40 to 60 years of age, sleep latency is approximately 17 minutes and sleep duration is 7 hours. From 60 to 70 years of age, sleep latency is 18 minutes and sleep duration is 6.2 hours.
During our 70s, sleep latency increases to 18.5 minutes and sleep duration is approximately 6 hours. From age 80 to the late 90s, sleep latency is approximately 19 minutes and sleep duration about 5.8 hours.
The need for 8 hours of sleep remains the same for all adults throughout the decades. Daytime naps usually offset the changes seen in sleep latency and sleep duration as we age.1
Insomnia Diagnostic Criteria
Insomnia, derived from Latin meaning no sleep, was originally thought of as a symptom but is now classified as a disorder in the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-V) and the International Classification of Sleep Disorders-Second Edition (ICSD-2).3
A diagnosis of insomnia from the DSM-V involves complaints of difficulty falling asleep, staying asleep, or experiencing non-restorative sleep. This inability to sleep is present despite adequate opportunity to sleep. The impairment in sleep leads to daytime distress and occurs >3 times per week and has been a problem for at least 1 month.
Finally, the diagnosis of insomnia disorder should occur in the absence of another sleep disorder or mental disorder. Insomnia disorder should not be the direct physiological effect of a drug or another medical condition.3
Insomnia can be further classified as short term when symptoms occur for <12 weeks.5 Chronic insomnia is when symptoms occur ≥3 times a week and for >3 months.5
Medications That Cause Insomnia
Pharmacists should be vigilant in recognizing medications that are causing insomnia in a patient's profile or electronic medical record (EMR). Medications that cause insomnia include antidepressants that are activating, such as bupropion and venlafaxine. Selective serotonin reuptake inhibitors, such as citalopram, fluoxetine, and paroxetine, are also activating.
Cardiovascular and respiratory medications that work as alpha agonists can cause insomnia. Stimulants such as amphetamines and methylphenidate can create sleep disturbances in young children.
Hormonal products including oral contraceptives, thyroid medication, and corticosteroids cause insomnia. Prescription products and OTC products containing caffeine, nicotine, and pseudoephedrine can keep you awake.6
Treatment Goals
The most important treatment goal for insomnia includes improvements in sleep quality and/or time. Relieving insomnia daytime impairment of energy, attention, or memory difficulties are another goal. Goals also include relieving cognitive dysfunction, fatigue, or somatic symptoms from insomnia.6
Nonpharmacologic Methods to Improve Sleep
Relaxation therapy including abdominal breathing, warm baths and hot showers, and massages may improve sleep. There is evidence indicating yoga, exercise, and meditation may improve sleep.
Making changes to your sleep environment including bed and bedding, noise, light, temperature, air quality, and clocks may alleviate sleep problems. Having a regular sleep pattern, eliminating daytime naps, avoiding alcohol, nicotine, and caffeine close to bedtime can improve sleep.
Acupressure, acupuncture, and homeopathic treatment options are also available. These treatment options can be mentioned when a patient prefers not to use prescription products, OTC products, or herbal remedies.7
Pharmacologic Therapies
OTC products
FDA-approved OTC products that treat insomnia include diphenhydramine and doxylamine. Nonprescription sleep aids are not indicated for patients suffering from chronic insomnia and a medical referral is recommended.8
Diphenhydramine and doxylamine are found in OTC pain medications and cold products. Pharmacists should discuss the possibility of duplicate therapy with consumers when consulting them on prescription medications for sleep.
Diphenhydramine
Diphenhydramine, a histamine 1 receptor antagonist marketed as Sominex and Benadryl, is found in products as 2 different chemicals, diphenhydramine HCL and diphenhydramine citrate. It is indicated for individuals 12 years of age and older and should be used for 2 days on and 1 day off to prevent tolerance.
Diphenhydramine peaks in the body in 2 hours and has an elimination half-life of 9 hours. Diphenhydramine HCL is dosed at 50 mg at night for adults, but some may benefit from 25 mg.
The dose for diphenhydramine citrate is 76 mg for adults. In children between 2 and 12 years of age, 1 mg/kg not to exceed 50 mg has been established as the appropriate dose. Previously, it had a pregnancy rating of B; however, using the new pregnancy and lactating rule, evidence in humans demonstrates a risk in the first trimester of pregnancy.9
Diphenhydramine should be used in caution with glaucoma patients because it can increase intraocular pressure. In 2019, the American Geriatrics Society recommended avoiding use of diphenhydramine and all first-generation antihistamines in the elderly.
Using anticholinergic medications can exacerbate symptoms of dementia and worsen cognitive decline in this group. Anticholinergic adverse effects (AEs) include dry eyes, blurred vision, urinary retention, dry mouth, and constipation.8
Doxylamine
Doxylamine is also found in several OTC sleep aids, in products such as Unisom. Reaching peak blood concentrations in 4 hours, doxylamine takes longer to take effect compared to diphenhydramine. It has an elimination half-life of 9 hours.8
Melatonin Supplements
Melatonin is considered a dietary supplement in the United States. There is evidence that it helps with sleep problems caused by jet lag and shift work. A 2013 review of studies on melatonin concluded that it may help people fall asleep faster, sleep longer, and sleep better. Long-term safety data have not been established.
The American Academy of Sleep Medicine does not recommend using melatonin in patients who have dementia or in geriatric medicine.10 OTC melatonin comes in 1 mg, 3 mg, and 5 mg.
A starting adult dose as low as 0.5 mg can aid in falling asleep. Melatonin crosses the placenta and reaches the fetus in many species and could affect the development of circadian rhythms.9 It is also transferred into breast milk.9
Herbal Products
Chamomile
Chamomile is derived from the Asteraceae plants, which are native to South and Eastern Europe. It is a natural sleep aid for insomnia and is available for purchase throughout health, grocery stores, and pharmacies in the United States.
Its formulations include powders, teas, tablets, and gel caps. It is hypothesized to work on gamma aminobutyric acid (GABA) receptors in the central nervous system (CNS) causing relaxation and sedation.11
Kava Kava
Kava Kava, also known as Piper methysticum, is found in the South Pacific and Polynesian islands. It has been used in Polynesian religious ceremonies, social events, and medicine.
The leaf and stem portions of the plant are poisonous, whereas the roots of the plant have some medicinal properties. In the United States, the inability to find standardized purified forms of the root extract has limited its use.12
Lavender
The effects of using lavender or lavandula angustifolia oil on the skin has been studied on sleep quantity and quality. A study published in the Journal of Alternative and Complementary Medicine indicates that the use of lavender oil is a safe and effective intervention to improve sleep. A systematic review of literature studies on the effects of inhaled essential oils on sleep concluded that they may be considered for people with mild sleep disturbances.13
Passionflower
Passiflora incarnata is an herbal sedative, anxiolytic, and popular sleep aid used for the treatment of sleep disorders, such as insomnia. A study was conducted using passionflower as an herbal tea in healthy adults.
Sleep was measured with diaries and included sleep quality measures. The study revealed that when used as an herbal tea, passionflower has short-term subjective sleep benefits.14
Valerian
Valerian is derived from the plant Valeriana officinalis. Its mechanism of action on relieving insomnia symptoms is unknown and it is not regulated by the FDA.
Evidence for valerian sleep is inconclusive and more research is needed to evaluate its use in insomnia. It is a safe medication and is approved for use as a food by the FDA. AEs of valerian root include gastrointestinal disturbances, drowsiness, headache, and nervousness.12 Safety data for long term use is unknown.10
Pharmacologic Products to Treat Insomnia
Benzodiazepines
Benzodiazepines work by binding to the GABA A receptors in the brain. When stimulated GABA receptors cause sedation, decrease anxiety, cause muscle relaxation, and have anticonvulsant activity. There are 5 benzodiazepines that are approved by the FDA to treat insomnia.
They include estazolam (ProSom), flurazepam (Dalmane), quazepam (Doral), temazepam (Restoril), and triazolam (Halcion). Onset and duration of action are important considerations, which influence prescribing.
Flurazepam and temazepam peak in the body in 1 to 2 hours and are a good recommendation for patients who have issues with sleep latency. Benzodiazepines approved for insomnia have long half-lives, with the exception of triazolam, and would be a good recommendation to increase sleep duration. Flurazepam and quazepam have active metabolites with very long half-lives and can contribute to daytime sleepiness and drowsiness.15
The American Geriatric Society does not recommend using benzodiazepines first when treating elderly patients. Benzodiazepines are not FDA-approved to treat insomnia in children or adolescents.
These medications have data that show teratogenicity in human pregnancy. Benzodiazepines are classified federally as schedule IV medications.15
Non-benzodiazepine Hypnotics
Non-benzodiazepine hypnotics, sometimes referred to as Z drugs, include zolpidem, zaleplon, and eszopiclone. These medications also work at the GABA A receptor in the brain and are specific to α1 on the GABA A receptor.
This specificity in binding, creates agonism at the GABA A receptor, which leads physiologically and biologically to sedative hypnotic properties only, making Z drugs exclusively for sleep.16
Zolpidem has different formulations, which include immediate (IR) and controlled release (CR) tablets, sublingual tablets, and an oral spray. Zolpidem IR tablets (Ambien) are made in 5 mg and 10 mg tablet strengths, with a half-life of 2.5 hours.
The CR formulation tablet strengths are 6.25 mg and 12.5 mg and are indicated for sleep latency and to increase sleep duration. The sublingual formulation marketed under the name Edluar comes in 5 mg and 10 mg.17
Intermezzo, another sublingual formulation, comes in 1.75 mg and 3.5 mg and is indicated for night awakenings.18 The 1.75 mg strength is indicated for women and 3.5 mg is indicated for men.18
Zolpimist is a cherry flavored oral spray that is packaged in a child-resistant container and must be primed before use. The adult dose for women is 5 mg and 5 mg or 10 mg for men. Each actuation delivers 5 mg of drug.19
Zolpimist is available in 4.5 ml and 7.7 ml spray bottles.19 All formulations of zolpidem are federally Schedule IV substances. Zolpidem has been associated with amnesia.
Human pregnancy studies with zolpidem have resulted in low birth weight and preterm deliveries. Zaleplon (Sonata) has a half-life of 1 hour and is sold in 5 mg, 10 mg, and 20 mg strength tablets.
Pregnancy data from animal studies show there is a risk of teratogenicity with zaleplon.9 Human pregnancy data indicate no risk in pregnancy, however, sample sizes in the study were small.9
Zaleplon is a federally scheduled IV substance. Eszopiclone (Lunesta) is the S enantiomer of zopiclone and works at the GABA A α2 & GABA A α3 receptor sites.16 Therefore, it has anxiolytic and sedative properties similar to benzodiazepines and can be prescribed for anxiety and insomnia disorders.
Eszopiclone 2 mg is indicated for sleep latency insomnia. Eszopiclone 3 mg is indicated to increase sleep duration in insomnia. Eszopiclone has human pregnancy data that indicate it is safe to use during pregnancy.9
Eszopiclone has been associated with an unpleasant metallic taste.20 AEs associated with Z drugs include headache and drowsiness.
Melatonin Agonists
Ramelteon, approved by the FDA in 2005, works in the suprachiasmatic nucleus (SCN) of the anterior hypothalamus. It is a melatonin agonist that binds to the MT1 and MT2 receptors in the brain.16 Ramelteon, which has 1 active metabolite, has a half-life of 70 minutes and reaches peak plasma concentrations in 60 minutes.
One advantage of ramelteon is that it does not have CNS depression effects. Chances of experiencing morning grogginess or a hangover feeling is unlikely. It is available in 8 mg tablets and patients should be instructed to take it 30 minutes prior to bedtime on an empty stomach.
It is not a controlled substance and previously had a pregnancy rating of C.21 Human pregnancy data are lacking.9
Melatonin is prescribed to children with insomnia at varying doses in Europe. A study published in the British Medical Journal further concluded that children given melatonin fall asleep earlier, but after 3 months of treatment wake up earlier.
It also determined that the major effect of melatonin is on sleep latency, rather than on total sleep time and doses of melatonin as low as 0.5 mg can be effective.22 Tasmelteon (Hetlioz) is a MT1 and MT2 receptor agonist.
The first FDA-approved therapy for non-24-hour sleep wake disorder in adults, tasmelteon was initially studied for the treatment of insomnia. In phase 2 and 3 trials, the compound received regulatory approval for non-24-hour sleep-wake disorder. It is also approved for sleep disturbances in children.
Tasmelteon should be taken on an empty stomach. It is supplied as 20 mg capsules and as an oral suspension with a recommended dosage for ≥16 years or ≥28 kg is 20 mg 1 hour before bedtime.
The dose for children 3-15 years of age or ≤28 kg is 0.7 mg/kg.23 In Europe prolonged-release melatonin (PRM) 2 mg/day is approved for treating insomnia in elderly patients. Endogenous melatonin declines as we age.
Data show that after 3 weeks PRM effects did not differ from placebo in all age groups. PRM significantly reduced sleep latency compared to placebo in elderly patients. There are good data that PRM is effective in the treatment of insomnia disorder in adults >55 based on 4 clinical trials.16
Doxepin
In 2020, doxepin was approved by the FDA marketed under the name Silenor to treat insomnia.24 Doxepin binds to the H1 receptor with high affinity and its antagonism at this receptor could be involved in its mechanism of action in increasing sleep duration. For adults, 6 mg can be taken within 30 minutes of sleeping, whereas for ages ≥65 years, 3 mg is recommended.24
Orexin antagonists
The newest medications to treat insomnia include orexin receptor antagonists. The orexin system, also called hypocretin, was discovered as a target for drug development and research for a new class of sleep medications. The orexin system directly innervates and excites noradrenergic, dopaminergic, serotonergic, histaminergic, and cholinergic neurons.25
The orexin receptor type 1 (OX1R) and 2 (OX2R) were studied in animals and adults. These medications are sometimes referred to as dual orexin receptor antagonists (DORA).16
In 2007, almorexant was found to induce sleep in mice, dogs, and healthy humans. In a phase 2 study, including adults and elderly patients with insomnia, almorexant dose dependently increased sleep latency and duration.
The orexin system and its function appear similar across human and animal species. The research results and discovery of almorexant led to the development of orexin receptor antagonists.26
The FDA approved orexin receptor antagonists for insomnia. Approval included suvorexant (Belsomra) from Merck in 2014, lemborexant (Dayvigo) from Eisai in 2019, and daridorexant (Quviviq) from Idorsia in early 2022.27
Suvorexant is a federally regulated Schedule IV substance that is dosed as 10 mg to be taken within 30 minutes of going to bed with at least 7 hours of time remaining before awakening. Patients should be instructed to take on an empty stomach and not to exceed 20 mg.
Suvorexant is available in 5 mg, 10 mg, 15 mg, and 20 mg tablets. Postmarketing surveillance has revealed adverse drug reactions that include palpitations, pruritus, and gastrointestinal disturbances. Pregnancy data from animal studies show decreased weight in pregnant mice and rabbits.
Lemborexant, a Schedule IV substance, is available in 5 mg and 10 mg tablets. The recommended starting dose is 5 mg taken within 30 minutes of going to sleep. It is preferable to take on an empty stomach. Studies have revealed that lemborexant is teratogenic in pregnant rabbits and mice.
Daridorexant comes in 25 and 50 mg tablets and should be taken 30 minutes prior to bedtime on an empty stomach. Headache is the most common AE reported with use of daridorexant.
Pregnancy data from animals indicate significant weight loss. Daridorexant has a half-life of 8 hours and studies indicate it may impair next day driving capabilities due to the residual effects of the medication. Daridorexant is pending a federal schedule at the time of this writing. Suvorexant, lemborexant, and daridorexant are metabolized by CYP3A4.28-30
Off Label Medications Used to Treat Insomnia
Mirtazapine
Mirtazapine 7.5 mg has been studied for insomnia in small clinical trials. It has been shown to increase total sleep time by a half-hour and reduces awakenings by 35%-40% compared to placebo.
Mirtazapine increases deep sleep stage N3, with subjects reporting that mirtazapine eased getting to sleep and improved sleep quality. Mirtazaine causes daytime sleepiness and lessened sustained attention.
Studies support the use of low-dose mirtazapine for the treatment of insomnia. Further studies are needed to gather data on the long-term effects and AEs. The mechanism of action of mirtazapine is through the histamine receptor.31
Trazodone
Studies indicate 50 mg of trazodone to be effective in improving sleep latency, wakefulness after sleep onset, and duration of sleep. Trazodone is approved in the treatment for depression and produces sedation via histamine receptors.5
Data with trazodone indicate it is safe to use during pregnancy. Specifically, congenital malformations are not likely based on studies conducted in pregnant females.9
Anticonvulsants
Gabapentin has data that show improvement in sleep efficiency and decreases in wakefulness after sleep onset. It can be used to manage insomnia in patients with alcohol dependence.
Pregabalin increases total sleep time, stage N3 sleep, and sleep efficiency. It reduces sleep onset latency and REM sleep. It is helpful in improving sleep in patients with anxiety disorders and fibromyalgia.5
Atypical antipsychotics
Olanzapine and quetiapine have sedative properties and low doses are prescribed off-label for sleep. Best practice guidelines from the American Family Physicians recommend not routinely using antipsychotic medications as a first-line intervention. If patients have a diagnosed psychiatric illness and experiencing insomnia, atypical antipsychotics are a good recommendation.
Drug Development and Research on Receptors Involved in Sleep
Receptors that are being investigated for drug development for the treatment of insomnia and other sleep disturbances include the histamine, adenosine (A), melatonin, serotonin, and dopamine receptors. The hormone melatonin is also being studied in other countries where it is a prescription product.
Agonism of the histamine 1 receptor is involved physiologically in waking. Antagonists such as diphenhydramine, doxepin, and amitriptyline bind to this receptor.
Adenosine is known as an endogenous sleep promoting substance. Adenosine analogs induce sleep when administered to animals. There are 4 adenosine receptors expressed in the CNS—the A1, A2A, A2B and A3 receptors.
The A1 and A2A receptors are involved in sleep and are being researched for the treatment of sleep disorders.16 These receptors have importance in regulating the depth and length of sleep.
Caffeine is an adenosine 2A receptor antagonist.32 Melatonin has been studied in Europe extensively and prescription medications of the hormone are used there. Agomelatine is a MT1 and MT2 agonist, and antagonist of 5HT2C receptor that is approved for depression in Europe and Canada.16
In the United States, MT1 and MT2 receptors are being investigated for drug development. Piromelatine is a MT1, MT2, and 5HT1A1D agonist that produces hypnotic and antinociceptive effects on EEG. Dopamine and serotonin are other drug targets for tranquilizers that cause sedation and are used to treat psychiatric disorders.16
In conclusion, there are several treatment options for insomnia and sleep disorders. Pharmacists can appropriately guide therapy in the management of insomnia and sleep disorders as they work with prescribing physicians. Pharmacists can also offer recommendations to consumers who have complaints about insomnia.
Using pharmacologic and non-pharmacologic treatments are the best approach in improving sleep disorders, such as insomnia. Research on the brain and sleep have led to the discovery of useful medications that aid in improving sleep.
Knowledge of new receptors and chemicals and the effects they have on the brain continue to be important areas in developing new therapeutic targets for sleep disorders.
Additional Resources on Sleep Research
References
1. Epstein, L., & Mardon S., The Harvard Medical School Guide to a good night's sleep, New York: McGraw Hill, 2007.
2. Kasbekar, R., & Ambizas, E., Helping People Manage Insomnia US Pharmacist. 2022; 1:4-12.3. Roth, T., Insomnia: Definition, Prevalence, Etiology, and Consequences. Journal of Clinical Sleep Medicine Supplement. 2007;3(5):7-10.
3. Roth, T., "Insomnia: Definition, Prevalence, Etiology, and Consequences." Journal of Clinical Sleep Medicine, Vol 3 Supplement 5, (2007):S7-S10.
4. Idzikowski, C., Sound Asleep The Expert Guide to Sleeping Well, London: Watkins, 2013.
5. Bollu,P., & Kaur, H., "Sleep Medicine: Insomnia & Sleep." Missouri Medicine, Vol 116, (2019): 68-75.
6. Schutte-Rodin S, Broch L, Buysse D, Dorsey C, Sateia M. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008; 4(5): 487-504.
7. DiGeronimo, T F., & Dimaria, F., Insomnia 50 Essential Things to Do, New York: Plume Penguin Group, 1997.
8. Berardi, R., McDermott, J., Newton, Gail. et.al. Handbook of Nonprescription Drugs an Interactive Approach to Self Care 14th Edition. Washington: American Pharmaceutical Association. 2004.
9. Miller, M., Mehta, N., Clark-Bilodeau, C., Bourjeily,G., "Sleep pharmacotherapy for Common Sleep Disorders In Pregnancy and Lactation" CHEST, Vol 157 (1), (2020): 184-197.
10. The National Center for Complementary and Integrative Health. "Melatonin What You Need To Know." Accessed online at www.nccih.nih.gov/health/melatonin-what-you-need-to-know. Accessed on February 9, 2022.
11. Yurcheshen, M., Seehuus, M., & Pigeon, W. "Review Article: Update on Nutraceutical Sleep Therapeutic and Investigational Research." Evidence Based Complementary and Alternative Medicine, New York: Open Access Article Under Creative Commons Attribution, 2015.
12. Davidson, J., & Connor, K., Herbs for the Mind, New York: The Guilford Press, 2000.
13. Lillehei, A., Halcon ,L., Savik, K., Reis, R., "Effects of Inhaled Lavender and Sleep Hygiene on Self-Reported Sleep Issues; A randomized controlled trial." The Journal of Alternative and Complementary Medicine, Vol 21, (2015):430-438.
14. Ngan A, Conduit R. "A double-blind, placebo-controlled investigation of the effects of Passiflora incarnata (passionflower) herbal tea on subjective sleep quality." Phytother Res. 25 Vol 8,(2011) 1153-9.
15. Matheson, E., & Hainer, B., "Insomnia Pharmacologic Therapy." American Family Physicians, Vol 96, (2017): 30-35.
16. Atkin,T., Comai, S., & Gobbi, G., Pharmacological Reviews, Canada & Italy: The American Society for Pharmacology & Experimental Therapeutics, 70:197-245, 2018.
17. Edluar (Zolpidem) Package Insert. Prescribing Information. Retrieved on February 11, 2022. Accessed online at www.accessdata.fda.gov/drugsatfda_docs/label/2014/021997s006lbl.pdf18. Intermezzo (Zolpidem) Package Insert. Prescribing Information. Retrieved on February 11, 2022. Accessed online at www.accessdata.fda.gov/drugsatfda_docs/label/2011/022328lbl.pdf
19. Zolpimist (Zolpidem) Package Insert. Prescribing Information. Retrieved on February 11, 2022. Accessed online at myzolpimist.com.
20. Lunesta (Eszopiclone) Package Insert Prescribing Information. Retrieved on January 29, 2022. Accessed online at www.lunesta.com.
21. Rozerem (Ramelteon) Package Insert Prescribing Information. Retrieved on January 29, 2022. Accessed online at www.rozerem.com.
22. Gringras, P., Gamble, C., Wiggs,L., Jones, A., et al. "Melatonin for Sleep problems in children with neurodevelopmental disorders: randomized double masked placebo controlled trial" British Medical Journal. Vol 345. (2012) Accessed online at www.bmj.com on January 29, 2022.
23. Hetlioz (Tasmelteon) Package Insert. Prescribing Information. Retrieved on January 30, 2022. Accessed online at www.hetlioz.com.
24. Silenor (doxepin) Package Insert. Prescribing Information. Retrieved on February 11, 2022. Accessed online at www.silenor.com.
25. Riemann, D., Krone, L. B., Wulff, K., & Nissen, C. "Sleep, insomnia, and depression." Neuropsychopharmacology Vol 45(1) (2020): 74–89.
26. Winrow C., & Renger J., "Discovery and development of orexin receptor antagonists as therapeutics for insomnia." British Journal of Pharmacology, Vol 171, (2014): 283-293.
27. Food and Drug Administration Sleep Disorders Sedative Hypnotic Information. Retrieved on January 29, 2022. Accessed online at www.fda.gov/drugs/postmarket-drug-safety-One attachment. Scanned by Gmail I information-patients-and-providers/sleep-disorder-sedative-hypnotic-drug-information.
28. Belsomra (Suvorexant) Package Insert Prescribing Information. Retrieved on January 29, 2022. Accessed online at www.belsomra.com.
29. Dayvigo (Lemborexant) Package Insert. Prescribing Information. Retrieved on January 29, 2022. Accessed online at www.Dayvigo.com.
30. Quviviq (Daridorexant) Package Insert. Prescribing Information. Retrieved on January 29, 2022. Accessed online at www.accessdata.fda.gov/drugsatfda_docs/label/2022/214985s000lbl.pdf.
31. Karsten J, Hagenauw LA, Kamphuis J, Lancel M. "Low doses of mirtazapine or quetiapine for transient insomnia: A randomised, double-blind, cross-over, placebo-controlled trial." Journal of Psychopharmacology. Vol 3, (2017 ):327-337.
32. Fisone, G., Borgkvist, A. & Usiello, A. "Caffeine as a psychomotor stimulant: mechanism of action. CMLS", Cell. Mol. Life Sci. 61, 857–872 (2004).
Questions
1. How does sleep change as we age?
A. Adults throughout every decade need 8 hours of sleep to function well
B. During adolescense, bed-wetting, night terrors, and sleepwalking occur
C. Sleep duration increases each decade as we age
D. Sleep latency decreases as we age
2. During non-REM (N) sleep:
A. Dreaming occurs
B. Growth hormone releases from the pituitary gland and stimulates tissue and muscle repair
C. Learning and memory are stimulated
D. Respiratory and heart rate increase
3. Which statement is correct regarding herbal products?
A. Lavender oil taken as 1 teaspoonful orally promotes sleep
B. The leaf and stem from the Kava Kava's plant produce anxiolytic and sedative properties
C. Chamomile and passionflower tea have sedative properties and can be recommended for mild sleep disturbances
D. The Asteraceae plant has safety issues such as hepatotoxicity, which limits its use
4. Which benzodiazepine is approved by the FDA for insomnia?
A. Alprazolam
B. Clonazepam
C. Estazolam
D. Oxazepam
5. A physician requests a recommendation for a patient who has insomnia and has abused sedative hypnotics in the past. The physician would like to prescribe a medication with no addictive potential. Which medication would be most appropriate?
A. Lemborexant (Dayvigo) 5 mg q hs
B. Eszopiclone (Lunesta) 1mg q hs
C. Ramelteon (Rozerem) 8mg q hs
D. Venlafaxine(Effexor) XR 75 mg q hs
6. A parent would like an OTC product for her 6 year old who has not been sleeping through the night for a week now. The child's prescription profile indicates recent prescriptions including an albuterol inhaler, loratadine, amphetamine and amoxicillin. How would you counsel this parent?
A. Discuss that amphetamine and albuterol could be causing insomnia and recommend diphenhydramine 25 mg at bedtime
B. Discuss that amphetamine and albuterol could be causing insomnia and recommend diphenhydramine 1 mg/kg at bedtime
C. Discuss that amphetamine and loratadine could be causing insomnia and recommend diphenhydramine 1 mg/kg at bedtime
D. Discuss that amphetamine and loratadine could be causing insomnia and recommend diphenhydramine 50 mg at bedtime
7. How does the mechanism of action of zolpidem differ from eszopiclone?
A. Zolpidem binds to GABA Aα1 receptor and eszopiclone binds to MT1 receptor
B. Zolpidem binds to MT1 receptor and eszopiclone binds to GABA Aα1 receptor
C. Zolpidem binds to GABA Aα1 receptor and eszopiclone binds to GABA Aα2 and GABA Aα3 receptors
D. Zolpidem binds to GABA Aα2 and GABA Aα3 receptors & eszopiclone binds to GABA Aα1 receptor
8. What is the most appropriate medication for a 76 year old male who can't fall asleep and is otherwise healthy?
A. Zolpidem 5 mg
B. Ramelteon 8 mg
C. Temazepam 15 mg
D. Diphenhydramine 25 mg
9. How should patients be counseled on lemborexant?
A. Take 30 minutes prior to bedtime and allow for 8 hours of sleep
B. Take on an empty stomach 2 hours before bedtime
C. Take with food to increase its effects
D. Take 30 minutes prior to bedtime and side effects include blurred vision
10. What do we know about adenosine receptors?
A. Caffeine is an adenosine 2A receptor agonist
B. Adenosine circulates in the body and causes wakefulness
C. There are 2 adenosine receptors in the CNS
D. Adenosine 1A & 2A receptors are involved in sleep regulation
Answer Key
1. A
2. B
3. C
4. C
5. C
6. B
7. C
8. A
9. A
10. D


Comments
Post a Comment